


Meniscal Tears Unmasked: Understanding the Differences Between Acute Trauma and Degenerative Damage
Nev Davies
Consultant Knee Surgeon
@nevtheknee
Meniscal tears are among the most common knee injuries, and they can occur due to various reasons, from sudden trauma to gradual wear and tear. Understanding the differences between acute traumatic and degenerative meniscal cartilage tears is crucial for appropriate diagnosis and treatment.
This blog explores these two types of meniscal damage, highlighting their causes, symptoms, and treatment options.
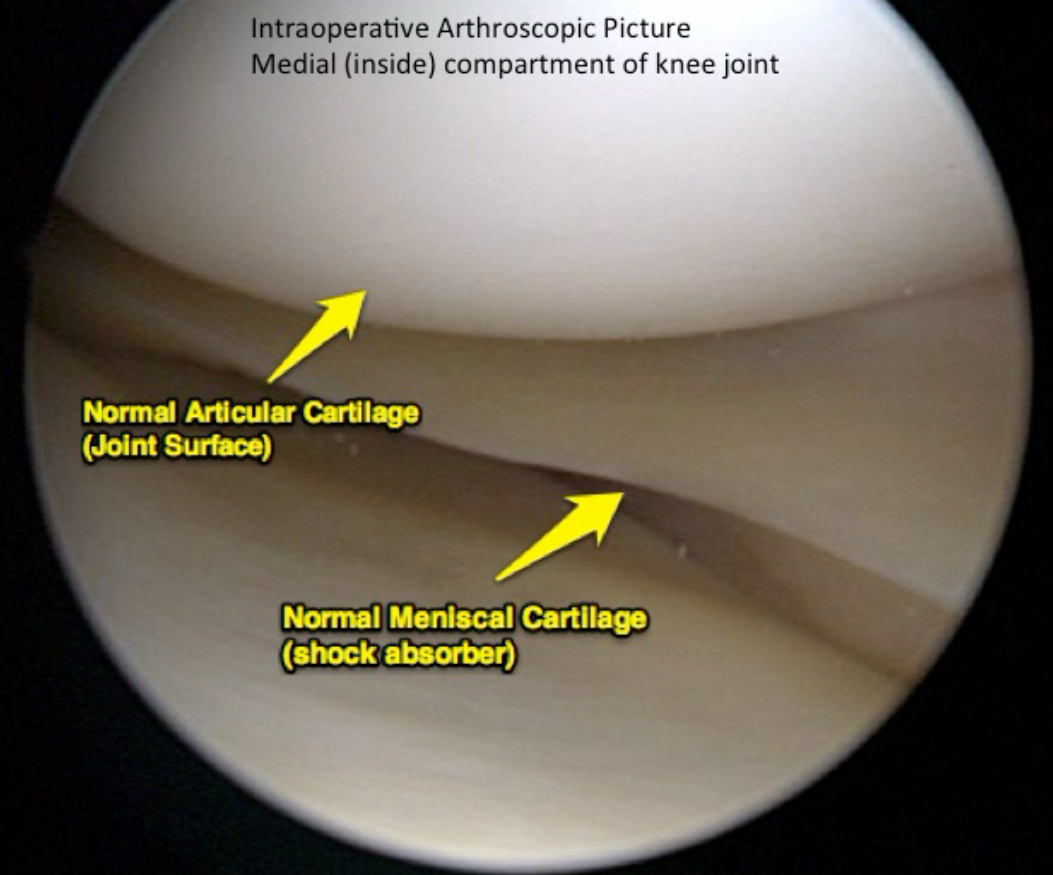
What is the Meniscus?
The meniscus is a wedge shaped piece of cartilage located in the knee joint. It acts as a cushion between the end of the thighbone (femur) and the top of the shinbone (tibia). Each knee has two menisci: the medial meniscus (on the inner side of the knee) and the lateral meniscus (on the outer side). These structures play a vital role in stabilizing the knee, absorbing shock, and distributing load during movement.
Acute Traumatic Meniscal Tears
Causes
Acute traumatic meniscal tears are usually the result of a sudden injury, often during activities that involve twisting, pivoting, or a direct impact to the knee. These types of tears are common in athletes, particularly in sports like football, rugby, netball, basketball, and skiing. The tear typically occurs when the knee is twisted forcefully while bearing weight.
Symptoms
The symptoms of an acute traumatic meniscal tear usually appear suddenly following the injury. Common symptoms include:
Immediate pain: Sharp pain at the time of injury, often localized on the inner or outer side of the knee.
Swelling:
The knee may swell within a few hours, indicating internal bleeding or fluid buildup.
Locking or catching:
The knee may catch or lock up, making it difficult to straighten the leg fully.
Instability:
A feeling of the knee giving way during movement.
Reduced range of motion:
Difficulty bending or straightening the knee completely.
Diagnosis and Treatment
Diagnosis of an acute traumatic meniscal tear typically involves a physical examination of the knee looking for swelling, range of motion, and joint line tenderness.
Imaging studies most often MRI are usually used to confirm the diagnosis.
Treatment depends on the severity and location of the tear, additional injuries and the patients individual circumstances
Options include:
Rest, Ice, Compression, and Elevation (RICE):
Initial treatment often involves RICE to reduce pain and swelling.
Physical Therapy:
Exercises to re-engage the muscles and strengthen the surrounding muscles and improve knee stability.
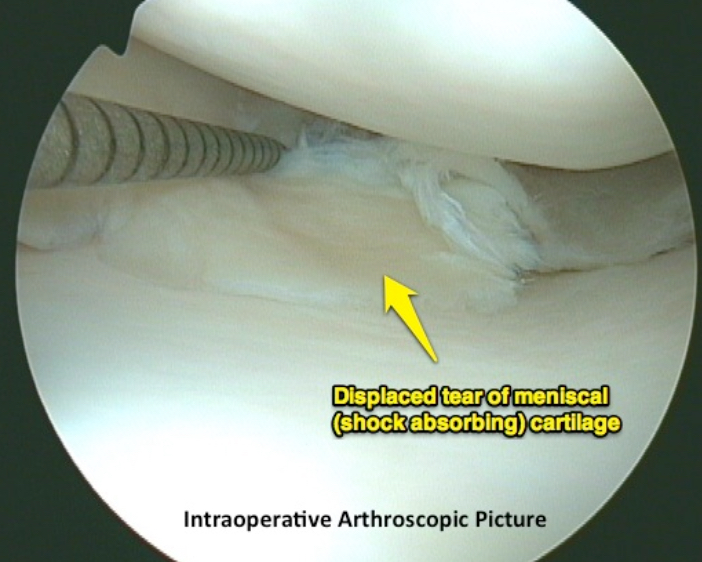
Surgery:
In some cases, particularly for large tears or displaced tears in young patients, arthroscopic (keyhole) surgery may be offered to attempt to repair or trim back the damaged portion of the meniscus. Post operative recovery depends on what was done during the surgery and the patient’s individual situation.
Degenerative Meniscal Tears
Causes
Degenerative meniscal tears are typically caused by the gradual aging and wear of the cartilage over time. These tears are more common in older adults, especially those over the age of 40, as the meniscus which is made up of springy collagen fibres naturally loses its elasticity and resilience with age. Degenerative tears are often associated with early osteoarthritis, where the joint surface cartilage wears down, leading to pain, swelling and stiffness.
Symptoms
The symptoms of a degenerative meniscal tear are usually more subtle than an acute tear and develop gradually. They may include:
Chronic pain:
Persistent, dull pain in the knee, often exacerbated by activity and relieved by rest.
Intermittent swelling:
The knee may swell occasionally, particularly after prolonged use.
Stiffness:
A feeling of stiffness or tightness in the knee, especially after periods of inactivity.
Mechanical symptoms:
Occasional catching or clicking in the knee, though these are typically less severe than in traumatic tears.
Gradual decline in function:
Over time, the knee’s range of motion and stability may decrease.
Diagnosis and Treatment
Diagnosis of a degenerative meniscal tear involves a physical examination and imaging studies such as MRI or X-rays to assess the extent of cartilage damage and the presence of any associated osteoarthritis.
Treatment for degenerative meniscal tears often focuses on managing symptoms and improving knee function, rather than surgical intervention.
Common approaches include:
Lifestyle modifications and time:
Avoiding activities that exacerbate symptoms, such as deep squatting or running on hard surfaces. Eventually the tear may settle with time and stop aggravating the knee completely.
Physical Therapy:
Strengthening exercises and flexibility training to support the knee joint. Muscles quickly disengage and loose control of the knee which exacerbates the viscous cycle of pain and weakness.
Medications:
Non-steroidal anti-inflammatory drugs (NSAIDs) help to reduce pain and inflammation.
Injections:
Corticosteroid injections may be used to relieve inflammation and pain and reduce the swelling inside the joint.
Surgery:
Surgery is less commonly recommended for degenerative tears, as the outcomes are generally less favorable compared to younger patients with traumatic tears.
Key Differences Between Acute Traumatic and Degenerative Meniscal Tears
1. Cause :
– Acute traumatic tears result from a specific injury, often involving a twisting motion or direct impact.
– Degenerative tears develop gradually due to aging and wear and tear on the knee cartilage.
2. Onset of Symptoms:
– Acute traumatic tears cause sudden and severe symptoms immediately after the injury.
– Degenerative tears cause symptoms that develop slowly and worsen over time.
3. Age Group:
– Acute traumatic tears are more common in younger, active individuals.
– Degenerative tears are more common in older adults, particularly those over 40.
4. Treatment Approach:
– Acute traumatic tears often require surgical intervention, especially in younger patients.
– Degenerative tears are typically managed conservatively with physical therapy, lifestyle changes, and medication.
Summary
Understanding the differences between acute traumatic and degenerative meniscal cartilage tears is essential for accurate diagnosis and effective treatment. While acute traumatic tears often occur in younger individuals following a specific injury, degenerative tears are more common in older adults due to the natural aging process.
Each type of tear requires a tailored approach to treatment, emphasizing the importance of individual care in achieving the best outcome. If you suspect a meniscal tear in your knee, I would be happy to see you for an accurate assessment, to organise and MRI scan and to work out a treatment plan.
Nev Davies FRCS (Tr&Orth)
August 2024





