

ACL – Anterior Cruciate Ligament (ACL) Reconstruction
Introduction – What is the ACL?
The ACL is one of the main structural ligaments that controls the stability of the knee, particularly in pivoting and side-stepping movements i.e. playing sports such as football, rugby and netball, as well as in dance and ballet. It also has important receptors (proprioceptors) within its tissue that gives clever, involuntary information to the brain and therefore helps the muscles control the knee. The ACL runs from the top of the notch in the femur (thigh bone), inwards and downwards to the front of the flat top side of the tibia (shin bone) (see picture 1).
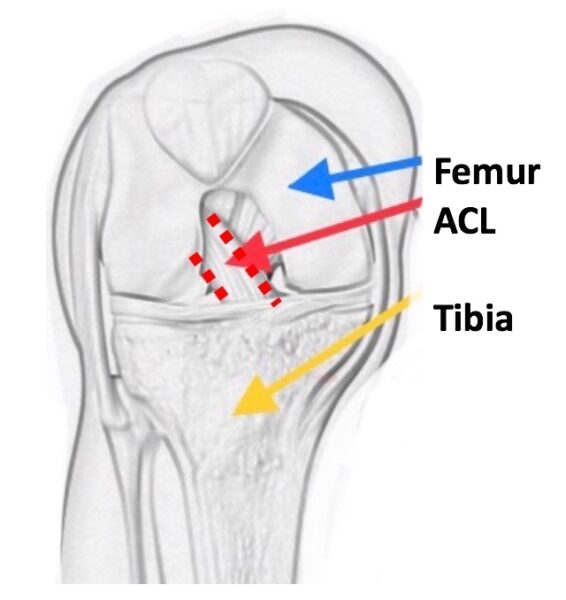
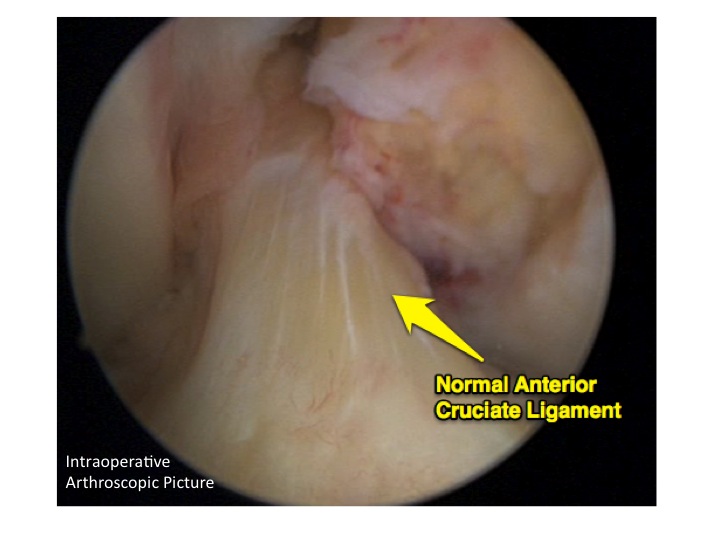
Picture 1a – sketch of ACL Picture 1b – arthroscopic (keyhole) picture of normal healthy ACL

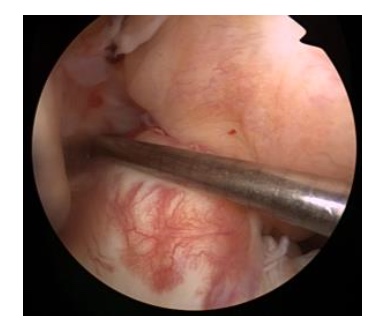
Picture 2a – twisting mechanism Picture 2b – ACL rupture at arthroscopy
Timing of Surgery
The timing of ACL reconstruction is variable depending on the individual situation. Factors that affect this timing include possible damage to other structures within the knee, particularly the meniscal shock absorbing cartilages (the cartilages between the knee bones) and also making sure the knee has been prepared by the physiotherapists i.e. the knee is ‘ready’ for the operation.
The preoperative physio sessions are crucial to ensure that:
1. The swelling has settled
2. The range of movement has returned to normal
3. The muscles have been reactivated, particularly the quadriceps muscles (the thigh muscles).
History of ACL Surgery
In the late 1970s and early 1980s some of the pioneers of ligament surgery started off by trying to repair these ruptured ACLs by essentially stitching them back together. Patients stayed in hospital for a week after surgery and were often in full leg plasters for up to 6 weeks! Orthopaedics has come a long way with the development of keyhole techniques, day–case units, enhanced recovery and emphasis on early rehabilitation. In those early days, the results were not that good, with only about one third of patients getting better and developing a stable knee. This meant repair techniques were quite quickly abandoned, and reconstruction (i.e. removing the damaged ligament and replacing it with a graft) came strongly into favour. Reconstruction quickly became the main surgical option for this injury in the late 1980s and remains so today.
What is involved with the surgery?
Over the last 30 years, ACL reconstruction surgery has been refined and improved tremendously. Nowadays surgeons perform lots of these operations and generally it is a particularly good procedure. It is done essentially ‘keyhole’ (this is where a small incision is made and fibre optics and special instruments are used to repair damage), takes about an hour to do, and patients go home the same day with crutches and a set of exercises to get the knee moving straight away. At the start of the operation, an examination under anaesthetic (EUA) reveals a very wobbly knee. (click here for a video showing a wobbly knee)
The first part of the operation is an arthroscopy (inserting a fibre optic camera) to look around and probe all the other structures within the knee to check they are normal and have not been damaged. This includes the articular surface cartilage of the joint (the smooth tissue that covers the ends of bones at joints) and the meniscal shock absorbing cartilages (the cartilages that absorb movement at the joint between the bones). Usually damage to these structures would be expected, as they are picked up on the MRI scan, but occasionally an associated injury is found at this time. Any issue identified can be dealt with there and then before beginning the ACL reconstruction. (Please read my additional information leaflet on meniscal injuries and chondral injuries here)
In 90% of my patients (children and adults) I use a hamstring tendon graft to reconstruct a new ligament. We collect two of the hamstring tendons from the same leg and having made special tunnels in both bones, we thread the tendons across the knee, forming a new ligament. They are held in place by a special fixation device (endobutton) in the femur (thigh bone) and a screw in the tibia (shin bone) in order to make the tension nice and firm. We fold them over to make a 4-string graft that is as strong as the original ligament. When I repeat the EUA at the end of the surgery, the knee is rock solid stable.
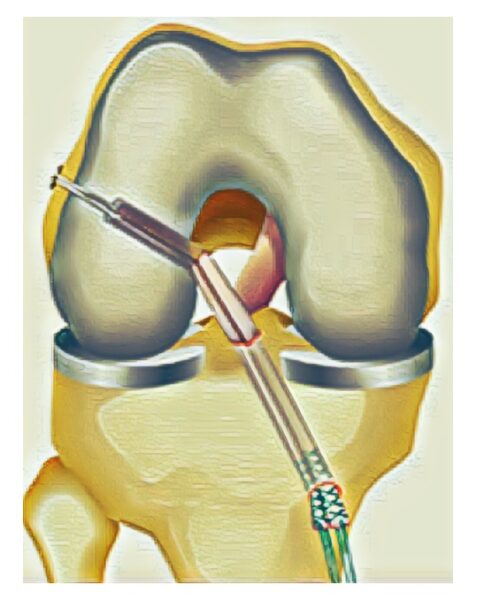
Picture 3: 4-String ACL Graft sitting across the knee
What is the after care ?
After waking up in the recovery you will come back to the day unit and rest with the leg elevated. At the end of the operation a wool and crepe wrap bandage is applied, snug but not tight. It should be worn for 48 hours and can then be reduced to a tubigrip dressing, which we give you to take home. The physios visit and when ready, get you up on crutches and confident hopping about. After you have been to the toilet successfully and have had something to eat and drink you will be able to go home (usually a few hours post operatively). It is advised to elevate the leg on pillows for the first 72 hours and to start gentle exercises as recommended by the physios. Ice packs (frozen peas wrapped in a tea towel will do) can help significantly with reducing swelling, bruising and can help with pain relief. Ice packs should be used for 10 mins at a time several times a day. State of the art compression cryocuffs (ice duvets) are available to hire in the post–operative period. (Click here for details) You should have regular pain killers – paracetamol and Ibuprofen together as per dosage instructions for at least 3-5 days.
What is the rehabilitation like after surgery ?
Rehabilitation is a big commitment postoperatively and gaining a good relationship and mutual trust of your physiotherapist is as important as with your surgeon. The time commitment is substantial and prolonged (12-18 months). It is only suggested you return to contact sports (match fitness) when you have satisfied all the specific return to sport criteria. This includes a barrage of strength, balance and flexibility tests on both legs to make sure the risk of re–injury to the operated leg but also the good leg is minimised. Returning to sport prior to this or not following the rehabilitation course puts the knee at massive increase of reinjury.
It is important to see your physio regularly to start with in the post–operative period. I see patients in my clinic at 6 weeks post op to check on early progress, go through my operative findings and pictures, and also get check X–rays to look at the tunnel positions. Further reviews are at 6 months and then 12 months post op to make a formal return to sport plan.
What are the success rates of surgery ?
As an honest UK knee surgeon, I tell all my patients undergoing an ACL reconstruction the following:
- the benefits of the surgery
- the likely natural history of the condition if we were not to do the surgery
- the non-operative alternatives
- the risks involved (both general risks with any surgery and specific risks to ACL)
- the likely success rates, particular the chance of returning to pre-injury level sports
In my hands, 80% of my patients having an ACL reconstruction get back to their original pivoting sports. Regarding re-injury and re-rupture of an ACL graft, the overall percentage quoted in the literature is around 5% but, unfortunately this is significantly higher (up to 25%) in the adolescent high-risk patient group. The other unfortunate fact is regardless of treatment path (operative or non-operative) 50% of patients will have developed some signs of early wear and tear in their knees (arthritis) at 10 years post injury, and hence are likely to have ongoing symptoms and problems in the future.
The National Ligament Registry
This is a UK database for patients undergoing ACL reconstruction in our country. It was designed by surgeons to enable accurate documentation of type of surgery, and outcome of patients following surgeries. These are called PROMS (patient reported outcome measures) Registries are powerful tools in medicine which help doctors to improve the care they can give to their patients. Although it is not compulsory, I strongly encourage my patients and families to allow us to enter your operative and follow up data. For more information visit the website, which is also a fantastic patient information resource. www.uknlr.co.uk
What are the risks of ACL reconstruction ?
General Risks of any surgery :
- Scars
Everyone (100%) gets a scar and most fade over time. Some patients with particular skin types can develop bumpy scars. - Pain, Bruising and Swelling (~90%)
Some slight discomfort and bruising is to be expected following every type of surgery. You will be given medication to control pain post operatively. Ice packs in the first 48 hours can help significantly.
An increased pain response (complex regional pain syndrome) has been reported in a few cases after ACL surgery but is very rare. - Numbness around the scars (~70%)
Some local numbness around the scar is normal and as things heal, it usually improves with time. - Infection (1-2%)
The wound sites may become infected. This usually settles with oral antibiotics. Very occasionally a further operation may be needed. Antibiotics are given at the time of the surgery and ‘deep’ infection within the knee joint is very rare. If this occurs a further operation would be required to wash out the joint. - Blood clots (Deep Vein Thrombosis) >1% in children)
These can occur in the lower legs following any surgery although are almost unheard of in children under 16 years old.
Specific Risks to ACL surgery:
- Graft rupture (5-25%)
The graft may rupture after further (often minor) trauma. Further surgery may then be necessary. (revision reconstruction) - Growth Disturbance (dependant on age of patient)
Any patient with growth remaining will be carefully monitored to check there is no uneven growth occurring. - Ongoing symptoms (mostly dependant on damage to other structures in the knee)
Persistent swellings, pain or mechanical symptoms may require further exploratory arthroscopy if not settling after several months. - Early Arthritis – 50% at 10 years
This is very dependent on lots of other variables, some controllable, some not.
I can’t emphasise enough how important it is to make sure we have gone through any questions you may have before we proceed with surgery.
In Summary
- Unfortunately, ACL injuries, particularly in youngsters are on the increase
- We see lots of young people with these injuries, sometimes associated with other damaged structures within the knee e.g. shock absorber cartilages
- Surgery is usually recommended for most young patients but not essential
- Rehab takes about a year to get back into competitive match sports
- Good pre and post-operative physio plays as big a part in outcome as good surgery
- Preventing reinjury and damage to the other leg is also key in the future
If you have any more questions please don’t hesitate to contact us now.





